CLSI 15 - 18 Jun 2019 AST meeting報告
(2019年6月15日~2019年6月18日:米国テキサス州ダラス)
大楠清文(東京医科大学)
2019年6月15日~18日に開催されたClinical Laboratory Standards Institute (CLSI)のAntimicrobial Susceptibility Testingミーティングに、日本臨床微生物学会から国際委員の大楠清文委員長(東京医科大学)が参加した。3日間にわたるプレゼンテーションおよびディスカッションが行われたので、決議事項を中心としてその概要をワーキンググループ別に報告する。なお、今回の会議で決定された事項については2020年1月のASTミーティングまでは最終ではなく、最終決定版はパブリックコメントを受けた上で2020年の1月に公表される予定である。

会議の前日に恒例となっているCLSI Education Workshop Presentationsが開催された。今回のトピックスはTo MIC or not to MIC, that is the question. Molecular Characterization of Antimicrobial Resistance (AR) for Healthcare in 2019と題して、3名の演者が各々臨床微生物検査室、公衆衛生、臨床の立場から以下の内容を中心として具体的な症例を例に挙げながらプレゼンテーションを行った。3名の演者のテーマと講演スライドをリンクするので、参考にしていただきたい。
- Clinical Microbiology Laboratory( PDF No.1)
- How labs are using and reporting molecular AST
- How to address in antibiograms - Public Health( PDF No.2)
- How PH labs are using molecular testing for outbreak in investigation and surveillance - Clinician( PDF No.3)
- Using results from molecular testing for AR to guide patient management
会議冒頭のOpening RemarksでChairholderのDr. Weinsteinから、M23に関するトレーニングセッションを開催したDr. WiklerとDr. Millerに謝意を表すること、淋菌に対するアジスロマイシンのブレイクポイント設定に関する学術的な根拠を発表(https://clsi.org/meetings/ast/rationale-documents/)したDr. HumphriesとDr. Castagnaに謝意を表すること、Outreach WGの活動においてASTニュースレター作成に貢献したDr. Schuetz, Ms. Hindlerに謝意を表すること、退職されるDr. Stephen Jenkinsの長年にわたる貢献に謝意を表すること、などが報告された。
Table 1ワーキンググループ
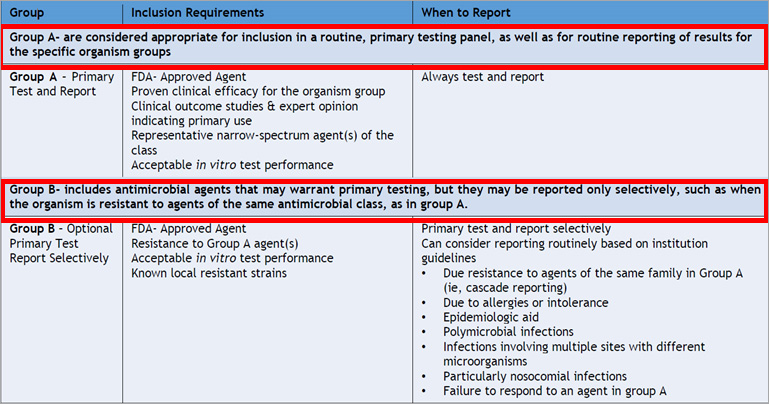
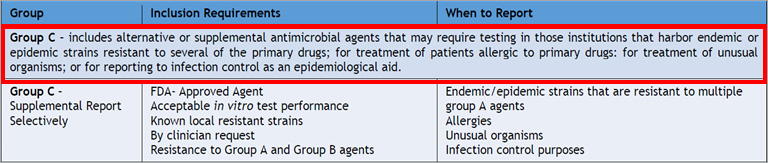
Table 1 のGroup A, B, Cの定義を以下のように明記すること、これらの詳細な記述を各グループの先頭に移動することが承認された。
※クリックすると拡大します。
※クリックすると拡大します。
Outreach Ad Hoc ワーキンググループ
最新トピックスを紹介するニュースレターとして、Volume 4, 2019年2号 Junが発刊(https://clsi.org/media/3174/clsi_ast_newsupdate_vol4issue2_june2019.pdf)されたことが報告された。
次号のニュースレター(2020年1号 Spring)は次の4項目の掲載が進行中であると報告された。
- Point-Counterpoint; Centralized vs. Decentralized AST Processing in Clinical Laboratories (workflow)
- A case study on Staphylococcus spp. not S. aureus
- Practical tips for fungal nomenclature
- A hot topic on Enterobacterales
次回のワークショップ(2020年1月)は以下のようなテーマで3領域の立場から講演が行われることが報告された。
Beyond SIR: Enhancing Laboratory Reports with Comments to Improve Understanding of the Report’s Intent.
- AST SC
- Antifungal Tests SC
- VAST
ブレイクポイントワーキンググループ(BPWG)
Colistin Breakpoint
腸内細菌目細菌(Enterobacterales)、Pseudomonas aeruginosa、Acinetobacter spp.のためのcolistinのブレイクポイントとコメントが以下のように承認された。なお、コメントは次項目のpolymyxin Bの内容も付記して記述する(M100 30th)。
| MICs (μg/ml) | |||
|---|---|---|---|
| Susceptible | Intermediate | Resistant | |
| Enterobacterales | - | ≤2 | ≥4 |
| Pseudomonas aeruginosa | - | ≤2 | ≥4 |
| Acinetobacter spp. | - | ≤2 | ≥4 |
Comments:
- Clinical and PK/PD data demonstrate this agent is of limited clinical efficacy.
- If available, alternative non-polymyxin agents are strongly preferred. If these agents are not available, this breakpoint presumes use of colistin and polymyxin B in combination with one or more additional, active antimicrobials.
- Isolates intermediate or resistant to colistin are intermediate or resistant to polymyxin B and vice versa.
- Colistin (methanesulfonate) should be given with a loading dose and maximum renally adjusted doses.
- When colistin or polymyxin B is given systemically, the drug is unlikely to be effective for pneumonia.
- Approved MIC methods include broth microdilution for colistin and polymyxin B, and broth disk elution and agar dilution for colistin. Gradient diffusion methods should not be performed.
Polymyxin B Breakpoint
腸内細菌目細菌(Enterobacterales)、Pseudomonas aeruginosa、Acinetobacter spp.のためのpolymyxin Bのブレイクポイントとコメントが以下のように承認された。
| MICs(μg/ml) | |||
|---|---|---|---|
| Susceptible | Intermediate | Resistant | |
| Enterobacterales | - | ≤2 | ≥4 |
| Pseudomonas aeruginosa | - | ≤2 | ≥4 |
| Acinetobacter spp. | - | ≤2 | ≥4 |
Comments:
- Clinical and PK/PD data demonstrate this agent is of limited clinical efficacy.
- If available, alternative non-polymyxin agents are strongly preferred. If these agents are not available, this breakpoint presumes use of colistin and polymyxin B in combination with one or more additional, active antimicrobials.
- Isolates intermediate or resistant to colistin are intermediate or resistant to polymyxin B and vice versa.
- Polymyxin B should be given with a loading dose and maximum renally adjusted doses.
- When colistin or polymyxin B is given systemically, the drug is unlikely to be effective for pneumonia.
- Approved MIC methods include broth microdilution for colistin and polymyxin B, and broth disk elution and agar dilution for colistin. Gradient diffusion methods should not be performed.
Stenotrophomonas maltophilia AHワーキンググループ
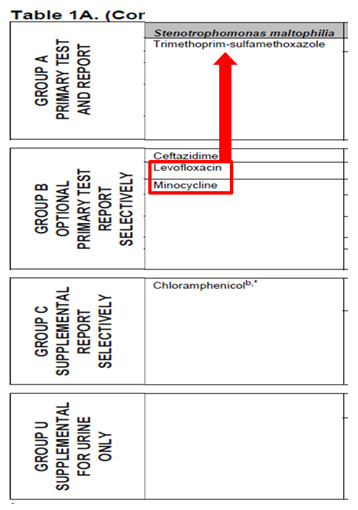
Stenotrophomonas maltophilia のTable 1のグループBに置かれていたlevofloxacinとminocyclineをTMP-SMXと同じグループAに移動させることが承認された。
Colistin Testing Methods AHワーキンググループ
腸内細菌目細菌(Enterobacterales)と緑膿菌(Pseudomonas aeruginosa)に対するコリスチンの新たな薬剤感受性試験法として2つの方法が検討された。10 mlのCAMHB液に10 μgコリスチンディスクを入れて実施するcolistin broth disk elution; CBDEとMHAにコリスチン0 , 1 , 2 , 4 μg/mLとなるように調整した平板を用いるcolistin agar test; CATの検討データが提示され、来年1月発刊予定のM100 30thに追加されることが承認された。各方法の詳細と検討データは PDF No.4を参照していただきたい。M100 30thのTable 3DにMethods for Testing Colistin Susceptibility for Enterobacterales and Pseudomonas aeruginosaのタイトルで追加される予定である。これらの方法に関する注意点とコメントのみを以下に転記する。
- The polymyxins (colistin and polymyxin B) are antimicrobial agents of last resort for treating multi-drug resistant infections. Clinical and PK/PD data suggest that these agents are of limited clinical efficacy. Alternative agents are strongly preferred. If these agents are not available, knowledge of the colistin MIC may be helpful to inform treatment decisions.
- Disk diffusion and gradient diffusion tests should not be performed for the polymyxins.
- Colistin and polymyxin B are considered equivalent agents so MICs obtained from testing colistin predict MICs to polymyxin B and vice versa. At this time, CLSI has not evaluated polymyxin B testing methods and the procedure below should not be adapted to polymyxin B. The methods below were evaluated for Acinetobacter spp. by CLSI and found to yield inaccurate results.
- These methods were established with limited disk and/or media manufacturers and are considered provisional until additional testing is performed to meet M23 guidelines.
Quality Controlワーキンググループ
今回の会議で以下の変更や削除等が承認された。
- E. faecalis ATCC 29212のplazomycinのQCレンジを削除する。
- E. faecalis ATCC 29212のaminoglycosidesのQCレンジを再検討する。
- E. coli ATCC 25922のディスク法のciprofloxacin QCレンジを29-38 mmに変更する
- Colistinの新たな薬剤感受性試験法(colistin broth disk elution; CBDEとcolistin agar test; CAT)のQC株としてE. coli AR Bank #0349を使用し、暫定的なQCレンジを1-4 μg/mLとする。
【M100 30thにおける語句の重要な変更点】
- Enterobacteriaceae(腸内細菌科細菌)がEnterobacterales(腸内細菌目細菌)と上位レベルに変更される。この変更は、2016年に腸内細菌目Enterobacteralesとこれに属する7つの科が新たに提唱されたためである。7科は、Enterobacteriaceae, Erwiniaceae, Pectobacteriaceae, Yersiniaceae, Hafniaceae, Morganellaceae, Budviciaceaeであるが、これまでのEnterobacteriaceae;腸内細菌科細菌に属していた菌種が他の科に移籍されたために表記をEnterobacterales(腸内細菌目細菌)と目レベルの階層まで広げる必要があった。例えば、Proteus属菌はMorganellaceaeに移籍され、Edwardsiella属菌はHafniaceaeに移籍された。この分類や名称が変更になった論文を PDF No.5として添付する。目(order)の名称が'Enterobacteriales'となっている文献やサイト等があるが、Enterobacteralesが正しい目名であることにも注意していただきたい。なお、目名の語尾は-ales、科名の語尾は-aceaeで終わることを覚えておくと学名がどの階層かを理解することができる。
- Coagulase-negative Staphylococcus spp.(CoNS)が“Other Staphylococcus spp.”の表記に統一される。
- “infection control”の語句が“infection prevention”に変更される。
次回のASTミーティング
次回のCLSI(Clinical and Laboratory Standards Institute) AST(Antimicrobial Susceptibility Test)ミーティングは、2020年1月26日~28日に、米国アリゾナ州テンピで開催されることが報告された。
(文責:大楠清文)
